 nl
nl
 Nederlands
Nederlands

DOREMY
What is the DOREMY trial?
The international DOREMY trial (NCT02106312) was initiated in 2010 for patients with myxoid liposarcomas (MLS), soft tissue tumors in the arms or legs. This study investigated whether a reduced dose of radiotherapy before surgery could be equally effective against this condition while minimizing side effects.
Patients received preoperative radiotherapy with a reduced dose of up to 18 x 2 Gy instead of the usual 25 x 2 Gy. One hundred patients participated in the trial, which was completed in August 2019.
What were the results of the DOREMY trial?
The median follow-up of the first 79 patients is now over two years. They have been treated for MLS with no metastases at the time of diagnosis. Local control at two years was 100%. When studied under the microscope, 91% of patients showed an extensive pathological treatment response to the reduced dose. Only 17% of patients experienced problems with wound healing after surgery, whereas a 35% chance would have been expected (historically) when opting for 25 x 2 Gy (see also O'Sullivan's SR-2 trial).
The full results of this trial were presented orally on November 12, 2020, during the annual Connective Tissue Oncology Society meeting (CTOS) and published in the leading journal JAMA Oncology. The results were presented by Jules Lansu, a PhD student working on this trial.
How did we reach these results and this study (prior experiences)?

The results of various studies over time
Division
The results of the various studies have been divided into 3 major phases:
Phase 1: 1990-2002: limb-sparing treatment (arms and legs)
Phase 2: 2002 -2010: radiotherapy-sensitive MLS (myxoid liposarcoma)
Phase 3: 2010-2020: Results DOREMY trial and where to go from here
Phase 1: 1990-2002 - limb-sparing treatment
The following achievements were made between 1996 and 2002:
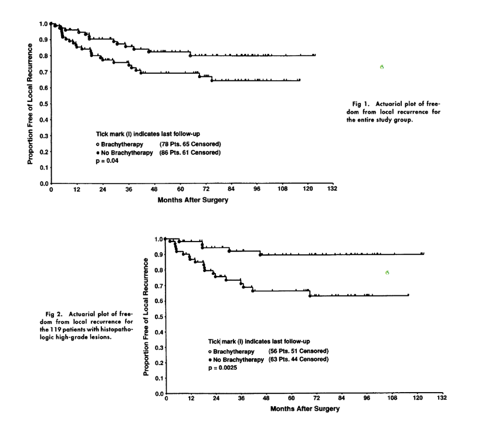
In 1996, the Memorial Sloan-Kettering Cancer Center sarcoma working group in New York, led by Peter Pisters and Murray Brennan, published the results of a prospective randomized phase III trial comparing the treatment outcomes of 86 patients receiving surgery with the results of patients who had both surgery and brachytherapy (internal radiotherapy).
Patients were followed for over 6 years on average. In the group that had only received surgery, the local control rates were 69%. This means that in 69% of patients who received surgery alone, there was no recurrence of the sarcoma in the affected leg or arm. In patients who received the combination treatment (surgery and internal radiotherapy), this was 82%.
The results observed in patients with high-grade sarcomas were even better. However, improvements in local control did not translate into an increase in survival (in other words, patients did not live longer on average).
(J Clin Oncol 1996;14:859-868)
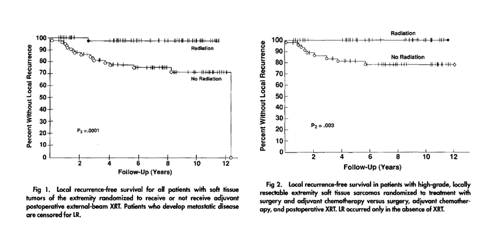
In 1998, James Yang and Steven Rosenberg from the National Cancer Institute, Bethesda, presented the results of a prospective randomized Phase III trial. Also in this trial, improvements in local control (the absence of a recurrence of the sarcoma in the affected body part) were observed in patients with low- as well as high-grade sarcomas after treatment with external beam radiotherapy and surgery, compared to treatment with surgery alone. Patients were followed 9.6 years on average.
(J Clin Oncol. 1998;16:197-203)
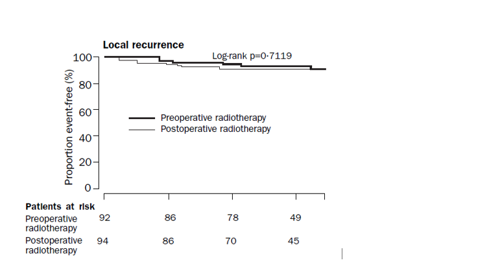
In 2002, Brian O’Sullivan from the Princess Margaret Hospital published the results of the important SR-2 trial, comparing the results of the standard postoperative radiotherapy in 94 patients with those of 88 patients receiving the new preoperative radiotherapy.
Below are the observed results. Patients were followed for 3.3 years on average.
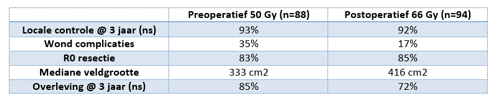
(ns = not significant)
(Lancet. 2002;359:2235-41)
Follow-up studies show that wound complications do not affect long-term functionality; quite the opposite, the group receiving postoperative radiotherapy experienced significantly more fibrosis, edema, and joint stiffness. (Int J Radiat Oncol Biol Phys. 2004;60:286-94. and Radiother Oncol. 2005;75:48-53.). More pathological femur fractures were observed in the postoperative radiotherapy group as well.
(Int J Radiat Oncol Biol Phys. 2009;75:1119-24.)
Phase 2: 2002 -2010 – Radiotherapy-sensitive MLS
After 2002, the focus shifted to the individual behaviors of the sarcoma subtypes.
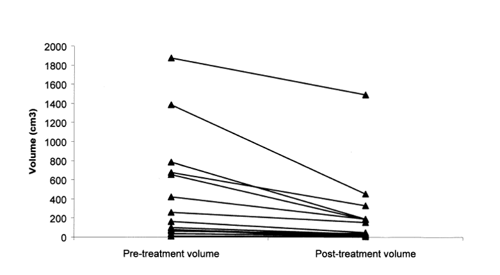
In 2004, Graham Pitson and Brian O’Sullivan (Princess Margaret Hospital, Toronto) were the first to observe that especially MLS tends to show an above-average radiosensitivity. Without exceptions, the MLS volume shrinks as a result of preoperative radiotherapy.
(Int J Radiat Oncol Biol Phys. 2004;60:522-6.)
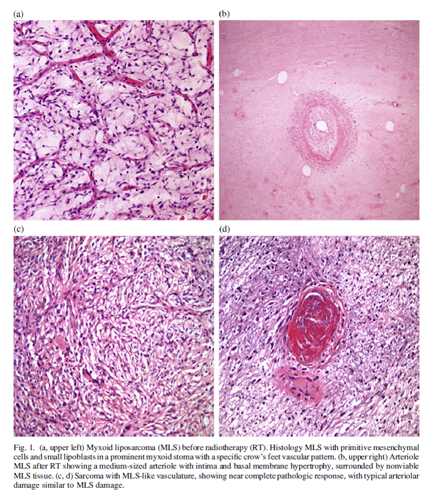
In 2007, Engström was the first to describe that this MLS volumetric response is associated with hyalinization and fatty maturation.
(Acta Oncol. 2007;46:838-45.)
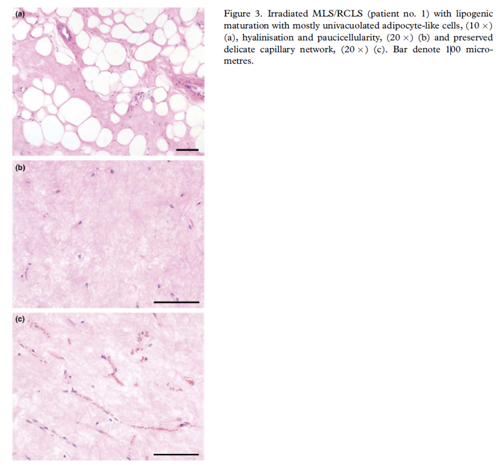
In 2008, Ronald de Vreeze – of our own sarcoma tumor working group – confirmed these pathological phenomena. He assumed arteriolar damage to be an explanation for the pathological response.
(Int J Radiat Oncol Biol Phys. 2008;72:1480-7)
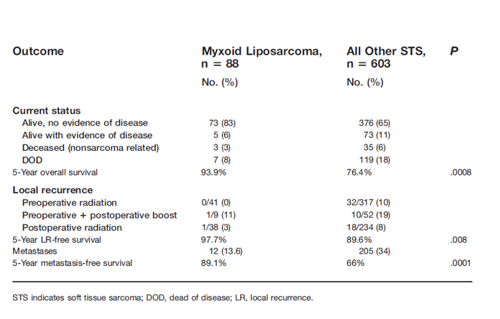
In 2009, Peter Chung found a correlation between radiotherapy sensitivity in MLS and an extremely high local control rate of 97.7% in 5 years in a group of 88 MLS patients.
(Cancer. 2009;115:3254-61.)
Phase 3: 2010-2020 - Results DOREMY study and how to proceed
In these previous publications (Pitson, Engström, De Vreeze, and Chung), the volume of the MLS tumor at the start of the treatment had been compared with the residual volume right before surgery, several weeks after completion of radiotherapy.
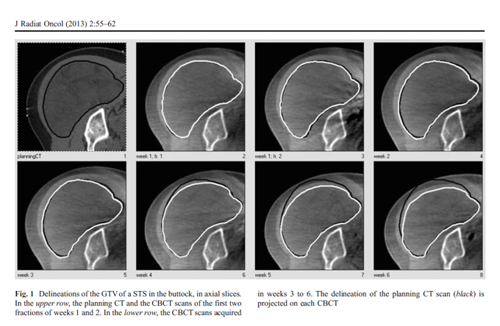
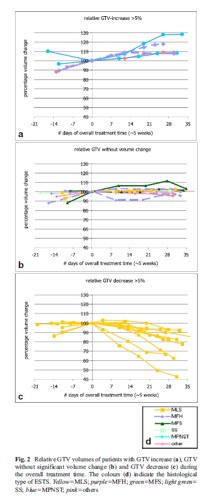
Anja Betgen of the NKI was the first to observe a decrease in volume as early as during radiotherapy in 2013. She investigated longitudinal imaging provided by the weekly cone-beam CT scan. This scan is intended to ensure that the patient is positioned correctly while receiving radiotherapy. Incidentally, the volume of the sarcoma can also be seen on this scan. Anja showed that the evident decrease in volume could already be observed as of the third week of radiotherapy, at which time a dose of only ~20 Gy had been delivered.
(J Radiat Oncol. 2013;2:55-62)
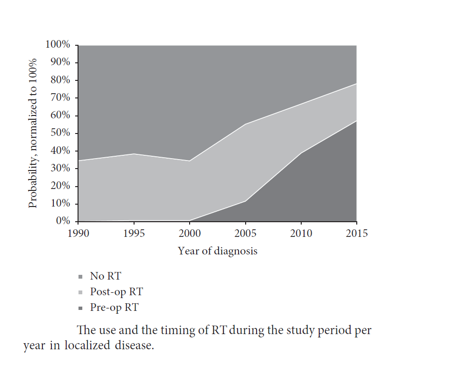
Based on research from the Netherlands Cancer Registry (NCR) supported by the Netherlands Comprehensive Cancer Organisation (IKNL) in 2020, Rick Haas and Jules Lansu presented that MLS patients are increasingly submitted to preoperative radiotherapy.
(Sarcoma. 2020:2437850.)
DOREMY
The international DOREMY trial (NCT02106312) was initiated in 2010. In this trial, MLS patients received a preoperative radiotherapy dose of only 18 x 2 Gy, instead of the standard 25 x 2 Gy.
The study closed in August 2019, when the 100th participant was registered. The results of the study were published on November 12, 2020, in the leading journal JAMA Oncology.
Where do we go from here?
As of mid-2021, sarcoma reference centers throughout the world started to participate in the DOREMY Registry (NCT04699292)
The results of the various treatment options for myxoid liposarcoma are prospectively registered in this database:
- surgery only;
- surgery in combination with various pre-operative radiotherapy dose schedules (25 Gy, 36 Gy, 50 Gy);
- surgery in combination with postoperative radiation (60-66 Gy);
- radiotherapy for symptom relief in case of metastases.
The goal of the database is to confirm that the results of the DOREMY trial apply to an even larger patient group.